Highlighting eating disorder awareness
Each February, National Eating Disorders Awareness Week brings communities together to spread awareness about eating disorders and share inspirational stories of hope and recovery. We are proud to stand with our nonprofit partners as we work together to shine a light on:
The serious, complex nature of eating disorders
The importance of accessing treatment
The power of believing that recovery is possible
How common are eating disorders?
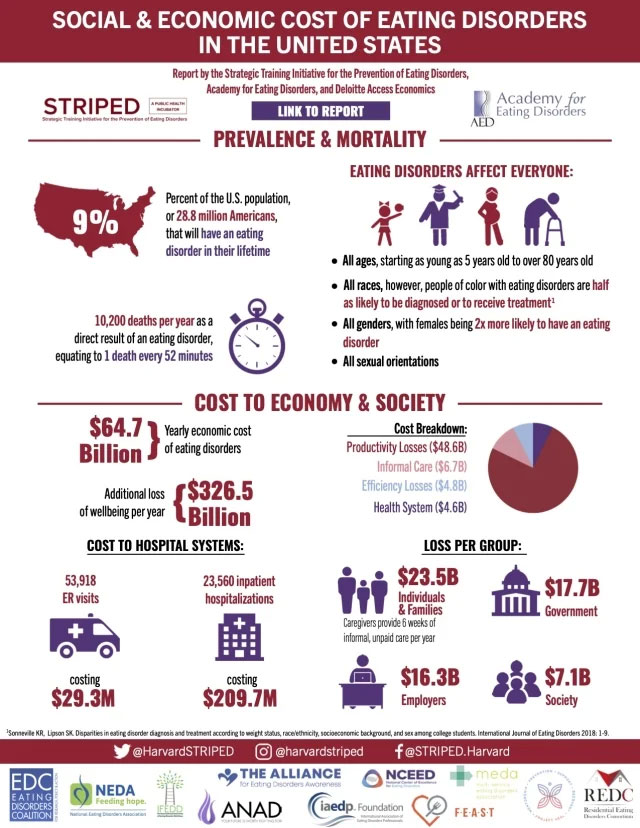
An estimated 9% of the U.S. population, or 28.8 million Americans, will have an eating disorder in their lifetime.[1]
In the U.S., 13%-21% of adolescent and young adult females may have an eating disorder. Binge eating and purging were the most common observed symptoms, increasing long-term health risks. [2]
In 2018-2019, nearly 2% of people in the U.S. (5.48 million people) were living with an eating disorder.[1]
Studies worldwide show that approximately 6%-8% of adolescents have an eating disorder[3] The incidence and impact of eating disorders among adolescents and young adults around the world increased between 1990 and 2021, with the highest burden and fastest growth affecting individuals aged 20-24.[4]
Eating disorder symptoms are seen in people of all ages. In women age 50 years and up:
13% have current eating disorder symptoms, most commonly binge eating and purging.
One in three say they have dieted “most of the time” over the past five years.
71.2% say they are currently trying to lose weight.
The vast majority (83.9%) reported being dissatisfied with their stomachs.[5]
The most common eating disorder in the U.S. as of 2019 was other specified feeding and eating disorder (OSFED).[1]
Eating disorders, gender and sexuality
Females are more likely to have an eating disorder, with 8.60% of females and 4.07% of males developing an eating disorder during their lifetime. This percentage is expected to rise over time.[1]
Eating disorders most commonly affect young women aged 20-29. Elevated rates are also observed among adolescents and women in their early 30s.[1]
In the U.S. in 2018-2019, approximately 1.09 million males (0.67% of males) had an eating disorder.[1]
The risk of eating disorders among college students grew by 13%, from 15% to 28%, between 2013 and 2021. The risk was most pronounced among female college students, Hispanic college students, and younger college students.[6]
Among college students, those who identified as the following had an increased risk of eating disorders:
Cisgender female
Bisexual
Queer
Questioning
“Other sexual orientation”
Gender-diverse[7]
View: Resources for LGBTQ+ individuals with eating disorders
Eating disorder mortality statistics
The statistics are sobering: In the U.S., one person dies every 52 minutes from an eating disorder.[1]
Approximately 10,200 deaths a year in the U.S. are a direct result of an eating disorder.[1] Estimates range from 5,500 to 22,000 a year.
All eating disorders increase mortality risk, particularly anorexia nervosa.[8,9]
In the U.S., eating disorder mortality rates are nearly six times higher for individuals with anorexia nervosa and nearly twice as high for those with bulimia nervosa, when compared to the general population.[1]
Individuals receiving inpatient care (hospitalization) for anorexia nervosa face a mortality risk greater than five times that of the average person, emphasizing the need for effective care.[10]
Those seeking treatment for bulimia nervosa and those in outpatient treatment for anorexia nervosa have twice the mortality risk as others.[10]
A full course of eating disorder treatment can reduce suicidal thoughts in those with eating disorders, offering protection.[11]
Read: Eating disorder relapse and recovery
What factors increase the risk of eating disorders?
Multiple research studies have identified a number of eating disorder risk factors, including genes, gender and sexuality, sexual trauma and more. Here are the stats.
Being female in the U.S. increases the risk of having an eating disorder.[1]
Having a close relative with anorexia nervosa can increase the risk for anorexia nervosa. Scientists have confirmed that anorexia can be inherited.[12]
LGBTQ+ individuals have an increased risk of an eating disorder. Out of 300,000 U.S. college students, those identifying as transgender, gay, lesbian or bisexual reported higher rates of disordered eating habits.[13]
Transgender males have higher levels of eating disorder symptoms than transgender women. Transgender women have higher levels of eating disorder symptoms than cisgender men. There is a trend of transgender men having higher levels of eating disorders than cisgender women.[14]
Surviving a sexual trauma can increase the risk of an eating disorder. Sexual trauma is uniquely associated with eating disorders, even when compared to other types of traumas.[15]
Life-changing events can increase the risk of eating disorders. At the start of the COVID-19 pandemic:
In the U.S and the Netherlands, those with a history of bulimia nervosa or binge eating disorder (BED) reported increased urges to binge eat and an increase in binge eating episodes.[16]
One-third of Australians with a history of eating disorders reported an increase in binge eating.[16]
Overall, the pandemic lockdowns were associated with increased eating disorder thoughts and behaviors, along with increased anxiety and depression.[17]
Anorexia nervosa statistics
Anorexia nervosa is one of the deadliest mental illnesses. The following statistics shed light on the importance of seeking help.
One study reported that among individuals with anorexia nervosa, one in five died by suicide.[18]
In the U.S., nearly all adolescents with anorexia nervosa feel socially impaired (88.9%). Nearly one in five (19.6%) feels severely socially impaired.[19]
The median age of onset for anorexia nervosa in the U.S. is 12.3 years, before the teen years begin.[19]
In the U.S., approximately 0.9% of women and 0.3% of men will have anorexia nervosa in their lifetime.[20]
Women with anorexia nervosa are twice as likely to have an alcohol use disorder than women without anorexia nervosa.[21]
If a close relative has had anorexia nervosa, one’s risk for anorexia nervosa is increased. Genetic factors account for more than half of the risk of anorexia nervosa.[22]
Bulimia nervosa statistics
Bulimia nervosa is slightly more common than anorexia nervosa. While bulimia has a lower mortality rate than anorexia, it still has very serious health consequences.
Of those with bulimia nervosa in the U.S., less than half have sought treatment for their eating disorder.[20]
In the U.S., approximately 1.5% of women and 0.5% of men will have bulimia nervosa in their lifetime.[20]
If a close relative has had bulimia nervosa, one’s risk goes up. Genetic factors contribute up to 75% of the risk of bulimia nervosa.[22]
Women with bulimia nervosa are two to three times more likely to be dependent on one or more of the following substances:
Cannabis
Stimulants
Cocaine
Alcohol[21]
Attention deficit/hyperactivity disorder (ADHD) is tied with bulimia nervosa. In a group of 57 females seeking treatment for bulimia:
They were far more likely to have symptoms of childhood ADHD (21%) compared to the general population (2.5%).
They were also more likely to have ADHD as adults.
Those with ADHD were more likely to have more severe eating disorder symptoms and more mental health symptoms.[23]
Individuals with bulimia nervosa are more likely to have a family history of suicide attempts. They are also more likely to have a mother who attempted suicide.[24]
In the U.S., bulimia nervosa is most likely to affect children aged 12.4 years, right around the time adolescence begins.[19]
Binge eating disorder statistics
Nearly 3% of U.S. adults will struggle with binge eating disorder. About 3.5% of women and 2% of men will have binge eating disorder in their lifetime.[20]
There is a genetic component to binge eating disorder. Research shows that it can run in families.[25]
Researchers studying specific eating disorders suggest that binge eating disorder has moderate heritability, typically estimated between 40% and 60%.[22]
While genes matter, environmental factors have a strong influence as well.[26]
Less than half of those with binge eating disorder have ever sought treatment specifically for their eating disorder.[20]
Following bariatric surgery:
25% of people still experience loss-of-control eating.[27]
5% of individuals still experience binge eating disorder.[27]
The median age of onset for binge eating disorder in the U.S. is 12.6 years, during early adolescence.[19]
ARFID statistics
Often considered an eating disorder of childhood, avoidant/restrictive food intake disorder (ARFID) affects people of all ages, genders and ethnicities.
ARFID affects more males than females.[28]
The true prevalence of ARFID is still being studied. A recent meta-analysis suggests it may affect as many as 4.51% of children.[29]
One study found that 5%-14% of patients in a pediatric inpatient eating disorder treatment program had ARFID while up to 22.5% of patients in a pediatric eating disorder day treatment program had ARFID.[28]
An inpatient treatment study from Johns Hopkins University found that underweight adults with ARFID gained weight at a slower rate than adults with anorexia nervosa. Adults with ARFID were also less likely to reach target weight goals.[30]
The same Johns Hopkins study also noted that patients with ARFID experienced fewer state anxiety and depression symptoms than those with anorexia nervosa.[30]
View more ARFID statistics here.
Diabulimia statistics
The medically recognized term for diabulimia is dual diagnosis of eating disorder and diabetes mellitus type 1 (ED-DMT1). Like all eating disorders, diabulimia stems from a combination of genetic, biological, psychological and sociocultural factors.
Females with type 1 diabetes have an increased risk of developing an eating disorder or disordered eating.[31]
The following factors may be signs of an eating disorder in adolescents with type 1 diabetes:
Poor glycemic control
Recurrence of hypoglycemic episodes
Calculating calories of foods/weighing foods
Missing medical visits regularly
Refusing to be weighed
Overly concerned with appearance
Preference for a vegetarian diet[32]
Eating disorders & co-occurring mental health disorders
Individuals with eating disorders and co-occurring mental health conditions often experience more distress than others. It is common for these individuals to need different psychotropic medications and different types of therapeutic interventions. Multiple rounds of treatment may be necessary, often making it difficult to stick to treatment and commit to recovery.
Approximately 9%-24% of individuals in eating disorder treatment have post-traumatic stress disorder (PTSD), likely leading to more severe symptoms.[33]
Eating disorders are significantly associated with substance use disorders.[21]
Autism and ADHD are more common in those with bulimia nervosa or binge eating disorder than in those without an eating disorder.[34]
Looking for more stats?
Get more facts about eating disorders and these specific co-occurring conditions at the links below:
We’re here for you when you need help.
These statistics can feel overwhelming. They also paint a picture of how serious and debilitating eating disorders can be.
But maintain hope. Treatment at Eating Recovery Center (ERC) has been shown to significantly stabilize weight and reduce depression, anxiety and psychological distress in children, adolescents and adults.[35]
At ERC, we are actively breaking the stigma around eating disorders. Our goal is to offer:
High-quality eating disorder treatment for those in need
Support for families and caregivers who need recovery resources
Education for professionals, equipping them to make the right decisions when referring their patients to a higher level of care
To learn more about eating disorder recovery, please fill out this form or call us at 866- 622-5914.